
The Measles Resurgence: A Behavioral Failure in Vaccination and Public Health Systems
By Jordan C Kabins, Ph.D., MBA
Introduction
Measles was officially declared eliminated in the United States in 2000, a major public health milestone made possible by widespread vaccination and the introduction of a two-dose strategy in the 1990s.
Recent data indicate a significant resurgence in measles cases, raising critical concerns regarding vaccination rates, behavioral compliance, public trust, and system-level preparedness.
A Preventable Disease Re-Emerges
The measles vaccine has been available since 1963, and with the addition of a second dose in 1990, effectiveness reached approximately 97% with two doses and 93% with one dose.
A notable measles outbreak occurred in 2019, when the United States reported 1,249 cases, the highest incidence since 1992. Of these cases, 89% involved individuals who were either unvaccinated or had unknown vaccination status, and 10% of the patients were hospitalized.
Despite this, a new outbreak is occurring:
2024: 285 cases
2025: 2,288 cases
2026 (current): 1,851 cases
The Threshold Problem: When Coverage Drops, Risk Accelerates
Measles is one of the most contagious diseases in the world. Herd immunity requires approximately 95% vaccination coverage.
However, recent trends show that the United States has been gradually using the MMR vaccine less often, and our health systems have not acted enough to change these public behaviors.
10-year average: ~93.3%
5-year average: ~92.3%
3-year average: ~91.9%
Although this decline appears minor, its impact is substantial.
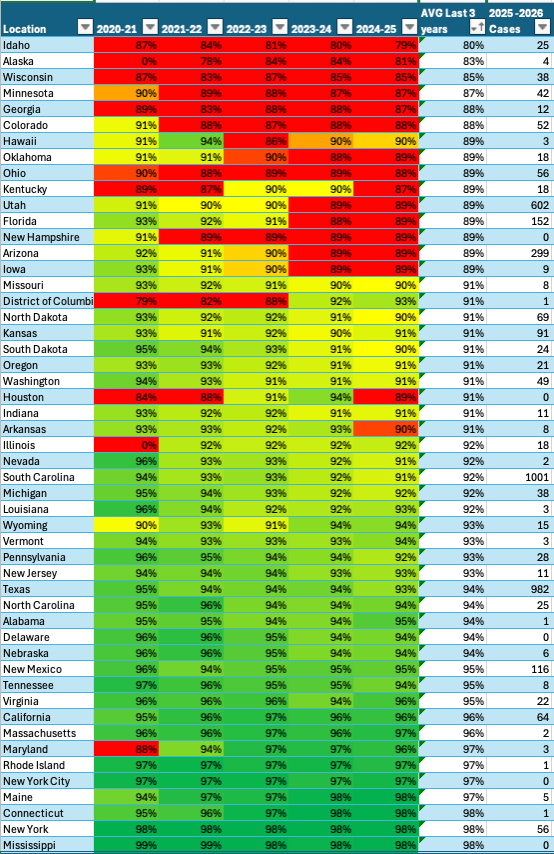
Table One provides a comparative view of vaccination performance, trend trajectories, and outbreak impact across locations during the 2025–2026 measles resurgence.
The data clearly demonstrate the following:
States 89% vaccination and below: 1,330 cases
States between 90–94.99%: 2,415 cases
States ≥95%: only 278 cases since 2025
This pattern does not represent a linear increase; rather, it reflects exponential risk escalation.
When vaccination rates fall below the herd immunity threshold, outbreaks are no longer isolated events. Instead, they become sustained and self-propagating.
A More Complex Reality: High-Vaccination States Are Not Immune To Outbreaks
Even states maintaining ≥95% vaccination rates are showing concerning trends.
Historically high-performing states like California and Virginia are seeing infections.
Why?
Herd immunity depends not only on overall vaccination percentages but also on the distribution of vaccinated individuals within the population.
For example:
California has seen increasing numbers of unvaccinated individuals:
18,940 (2022–2023)
21,648 (2023–2024)
23,043 (2024–2025)
Localized gaps in vaccination coverage create pockets of vulnerability, enabling outbreaks to occur even in states with otherwise high overall vaccination rates.
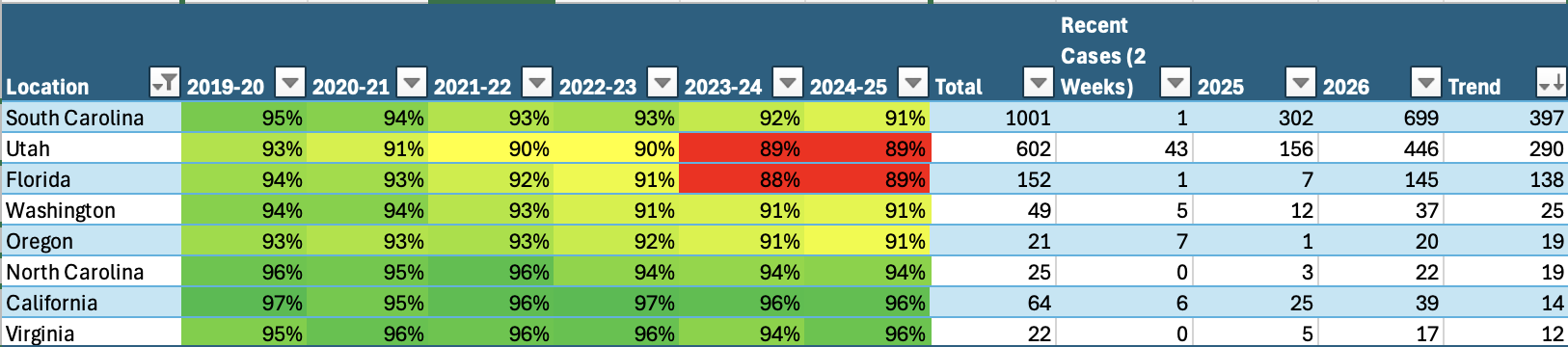
Table Two highlights states with increasing measles incidence in 2026 compared to 2025, including high-performing vaccination states that continue to report active cases.
Temporary Improvement ≠ Long-Term Control
Some states, like Texas and Arizona, show fewer cases in 2026 compared to 2025.
However, this reduction should not be interpreted as a resolution of the underlying issue.
Both states have suboptimal vaccination rates and they still report recent active cases
This reflects a dangerous dynamic:
Outbreaks may be temporarily controlled
However, outbreaks remain structurally likely to recur in environments with low vaccination coverage.
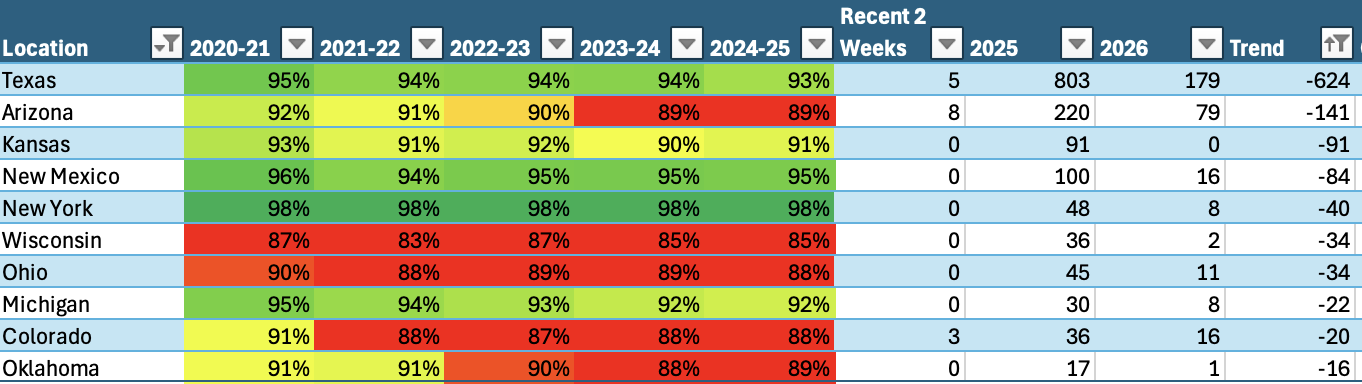
Table Three identifies states with reduced measles cases in 2026 compared to 2025, while emphasizing that they remain in active outbreak conditions.
It is important to note that the United States reported 1,274 measles cases in 2019 and only 13 in 2020, suggesting that affected areas were able to quickly control and end the outbreak.
What Needs to Happen Next
1. Rebuild Vaccination Momentum
Vaccination rates must not just improve; they must consistently exceed the herd immunity threshold.
2. Strengthen Healthcare System Response
Healthcare providers must:
Improve early detection
Strictly follow infection control protocols
Contain the spread immediately
3. Address Behavioral Drivers
Policy interventions alone are insufficient to address the current challenges.
It is necessary to address the following factors:
Vaccine hesitancy
Misinformation
Trust in healthcare systems
Risk perception
4. Target High-Risk States and Trends
States with declining vaccination rates, such as:
Utah
Florida
Arizona
Oregon
California
Texas
Washington
South Carolina
These states must be prioritized for targeted intervention.
Measles is not returning because we lack the tools to prevent it.
It is returning because:
Vaccination behaviors are declining
Compliance systems are weak. This issue is no longer solely a clinical problem; it has become a behavioral and systems-level challenge.
Reference:
Centers for Disease Control and Prevention. (2026). Measles cases and outbreaks. Centers for Disease Control and Prevention. https://www.cdc.gov/measles/data-research/index.html#cdc_data_surveillance_section_5-yearly-measles-cases
Johns Hopkins University. (2026). U.S. measles tracker | International Vaccine Access Center. U.S. Measles Tracker. https://publichealth.jhu.edu/ivac/resources/us-measles-tracker
Kabins, J. (2026). The Challenges and Experiences of Mask Compliance among Nurses in Southern Nevada during COVID-19.